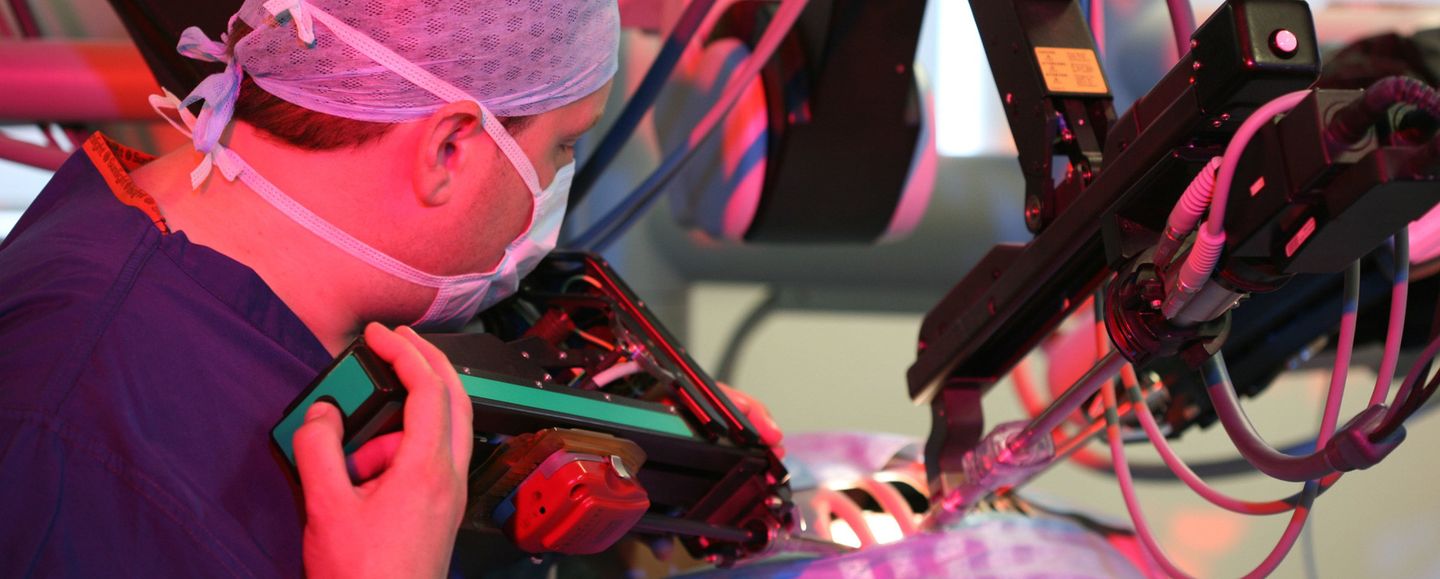
Surgery
The Division of Surgery aims to improve outcomes for patients undergoing surgical treatment of disease through the transfer of technology into clinical practice. This is being achieved by harnessing Imperial College’s interdisciplinary research strengths and by bringing together clinicians, engineers, designers, and policy makers to create highly innovative solutions across seven broad themes.
Find out more